In case you haven’t noticed there have been some rather ambiguous statements made by the Centers for Disease Control and Prevention recently regarding previously accepted standards for certain vaccines for infants.
The most recent of these statements and recommendations come from the CDC’s Advisory Committee on Immunization Practices. Specifically, they are referring to the hepatitis B vaccine for infants. The committee voted to make vaccine recommendations “based on the mother’s testing status.” So, if a mother tested negative for hepatitis B parents should decide, with the guidance of their doctor, whether the vaccine is appropriate for their newborn.
The Los Angeles Department of Public Health (DPH) criticized the decision and described it as “a return to selective, risk-based newborn vaccination”, which officials argued was “not based on new evidence suggesting that hepatitis B vaccine birth dose is unsafe or ineffective.” The DPH further argued that a “risk-based strategy” was shown to be inadequate more than 35 years ago, and can reintroduce preventable risks, in particular communities such as L.A. County where hepatitis B prevalence and risks are higher. Consequently, the county has decided to continue the current, science-based recommendation for hepatitis B vaccines for newborn.
To keep this in context, the new CDC recommendations are occurring while other vaccines for newborns are also being brought into question, in particular, the vaccine for measles which has also been questioned by the new CDC while there have been outbreaks in several U.S cities.
House Representative, Judy Chu, D-Pasadena, a member of the House Ways and Means Committee and Chair emerita of the Congressional Asian-Pacific American Caucus, criticized the CDC’s decision as “reckless and dangerous.” She added: “Asian Americans, Native Americans and Pacific Islander communities who make up only 7% of the U.S. population yet account for 60% of chronic hepatitis B cases. She argued that these vaccines have been life- saving protection for these communities.”
We strongly continue to suggest that all expectant and recently delivered parents speak frankly and honestly with their pediatricians regarding newborn vaccines for their newborn.






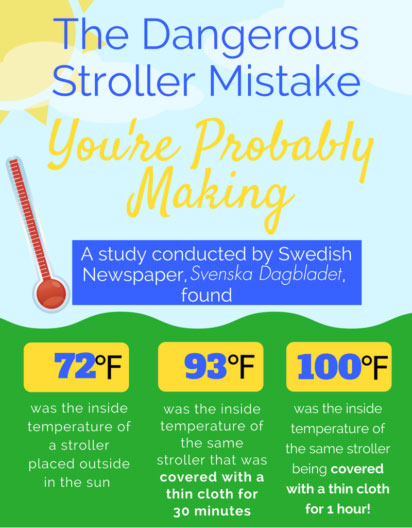 Based on an interview with Stockholm pediatrician Dr. Svante Norgren about the dangers of covering a stroller, the Swedish newspaper, Svenska Dagbladet, conducted an experiment by putting a stroller out in the sun, midday, in the summer. Without a cover, the stroller was about 72 degrees Fahrenheit. After covering the stroller with a thin cover for 30 minutes, the temperature rose to 93 degrees and after an hour, 100 degrees!
Based on an interview with Stockholm pediatrician Dr. Svante Norgren about the dangers of covering a stroller, the Swedish newspaper, Svenska Dagbladet, conducted an experiment by putting a stroller out in the sun, midday, in the summer. Without a cover, the stroller was about 72 degrees Fahrenheit. After covering the stroller with a thin cover for 30 minutes, the temperature rose to 93 degrees and after an hour, 100 degrees! Dress children lightly, use plenty of sunscreen, and keep them well-hydrated. Sponge your child with a damp cloth to keep them comfortable. A small clip-on fan can be attached to their stroller for added circulation – just be sure to keep it out of reach.
Dress children lightly, use plenty of sunscreen, and keep them well-hydrated. Sponge your child with a damp cloth to keep them comfortable. A small clip-on fan can be attached to their stroller for added circulation – just be sure to keep it out of reach.