A coordinated effort between the American Academy of Pediatrics and the American Heart Association has produced new CPR and airway obstruction guidelines which went into effect towards the end of 2025. This is an important update and one all families should be aware of.
CHANGES FOR INFANT CPR
The use of two or three fingers on the chest for compressions is no longer in effect. It is now recommended that the rescuer use the palm of their hand between the nipples (as before),

or alternatively, the two-thumb encircling hands technique.
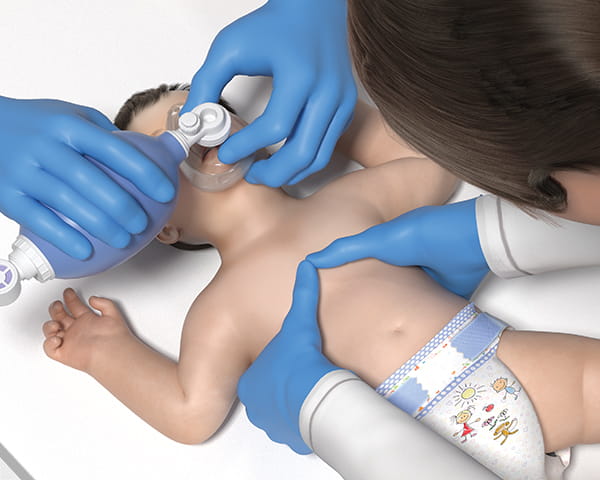
We still need to move the infant chest at least 1/3 of its depth or about 1.5 inches. The ratio of pumps to breaths remains 30 pumps and 2 rescue breaths.
This change reflects the fact that most rescuers were not pumping deep enough.
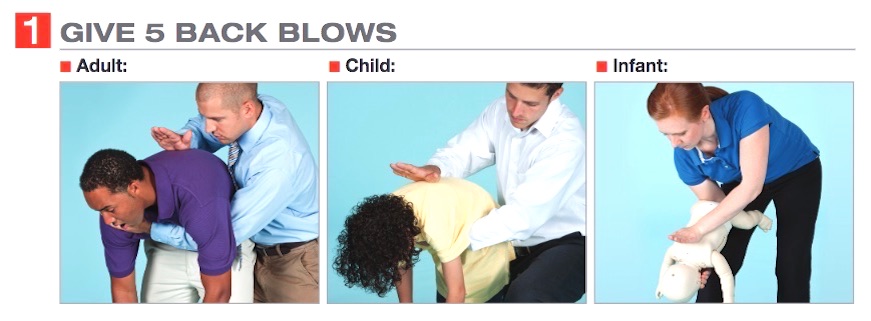
The recommendation for foreign body obstruction (choking) is unchanged. Repeated upper back hits (up to 5) followed by up to 5 chest thrusts is still the method of choice until the baby is over one year old.
CHANGES FOR CHILD CPR
CPR technique for a child now includes the use of two hands to ensure adequate depth of compression (at least 1/3 of the chest wall depth).
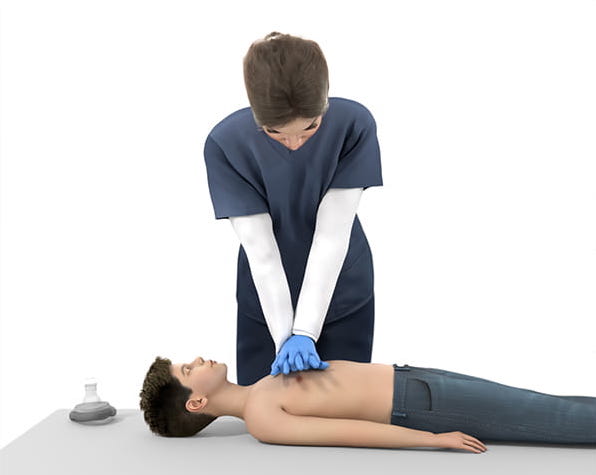
Please remember that if a child is no longer conscious due to airway blockage it is imperative that CPR begin immediately.
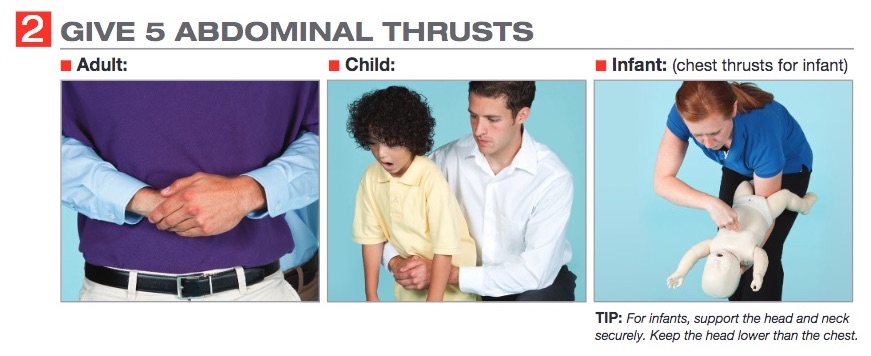
The new recommendation for a choking child now includes 5 upper back hits followed by up to 5 abdominal thrusts (inward and upward), alternating until the object is cleared.
- For best effect, position yourself to the side and slightly behind the choking child. For a small child, you may need to kneel behind them rather than stand. This should be done while the child is bent over. Previously we suggested back hits while the child was standing upright.
- Give 5 back blows using the heel of the hand to strike between the shoulder blades. If no improvement, then have the child stand up straight.
- Next, move behind the child; bend your knees slightly for balance and support, and give 5 abdominal thrusts, pulling inward and upward each time.
- Continue alternating 5 back blows and 5 abdominal thrusts until the child can cough, cry or speak.
- If they become unresponsive, begin CPR (starting with compressions)
CORRECT RESPONSE TO CHOKING
As always, we continue to encourage parents and care providers to follow the basics of prevention of airway obstruction by adhering to the following principles:
- Never leave an infant or small child unattended during mealtimes
- Once they are crawling/walking keep all food and other objects away from them
- Do not provide food or snacks in the car as it is difficult or impossible to recognize an airway obstruction before it is too late
- Be extra careful if you enter a small mouth to try and remove an object. If you must, do so by going along the cheek then swipe across the mouth
When someone is choking immediate response is crucial. You can’t rely on Paramedics to save the day as they won’t be able to arrive in time. That is why we cannot stress enough how important it is for ALL family members and care providers to know how to save a choking infant or child.
BE PREPARED. BE SAFE.






 Rebecca Payne, one of the study’s authors, said it could be dangerous to rely solely on this new technology which might fail to recognize when a person needs urgent medical attention.
Rebecca Payne, one of the study’s authors, said it could be dangerous to rely solely on this new technology which might fail to recognize when a person needs urgent medical attention. As for the rest of us who are still largely flying by the seat of our pants, it’s probably best to continue to rely on traditional doctor/patient interaction, at least for the time being.
As for the rest of us who are still largely flying by the seat of our pants, it’s probably best to continue to rely on traditional doctor/patient interaction, at least for the time being.









